
How to calculate air exchanges per hour (ACH) in an operatory with an in-operatory air cleaner (HEPA filter unit):
The typical dental operatory has an area 100 square feet with an 8 foot ceiling, which gives a volume of 800 cubic feet.
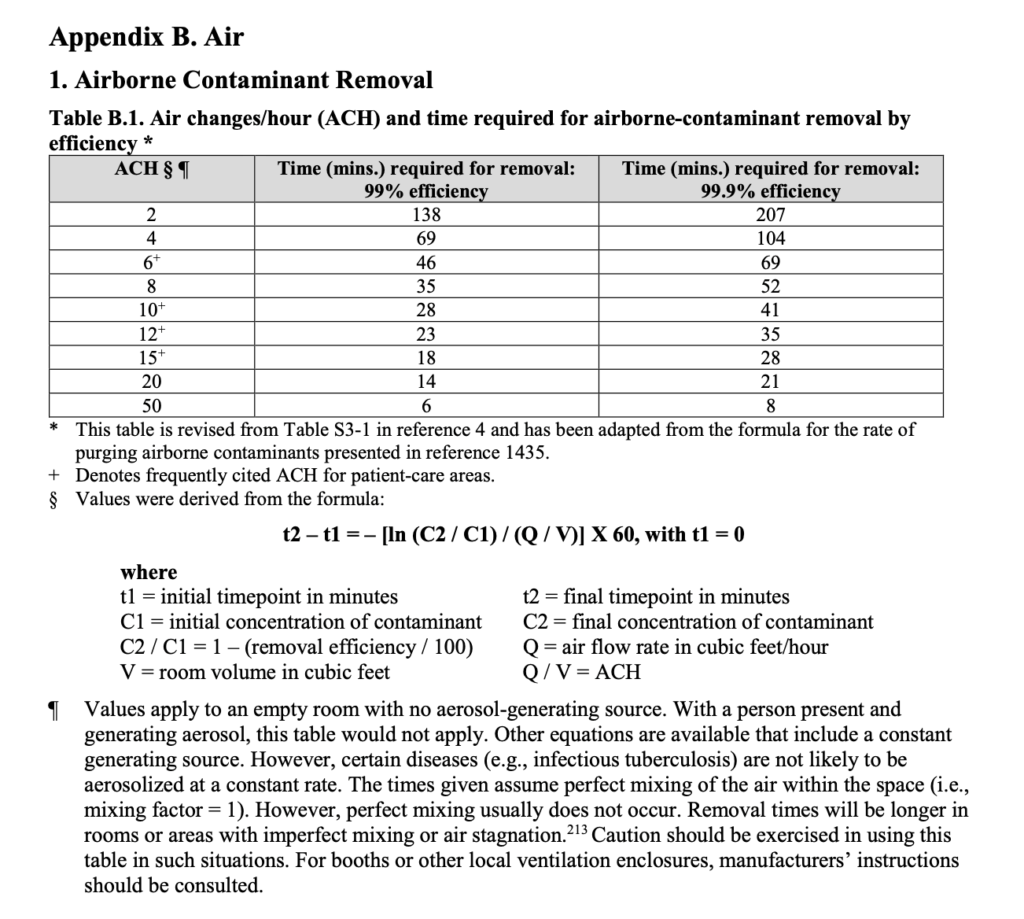
Following an aerosol generating procedure, the operatory must be left empty to permit clearance and settling of aerosols for a length a time determined by the air changes per hour (ACH) and the formula : t2 – t1 = – [ln (C2 / C1) / (Q / V)] X 60, with t1 = 0

Now available: Advanced HEPA Air Purifier Berk D9L
The typical dental operatory has an area 100 square feet with an 8 foot ceiling, which gives a volume of 800 cubic feet.
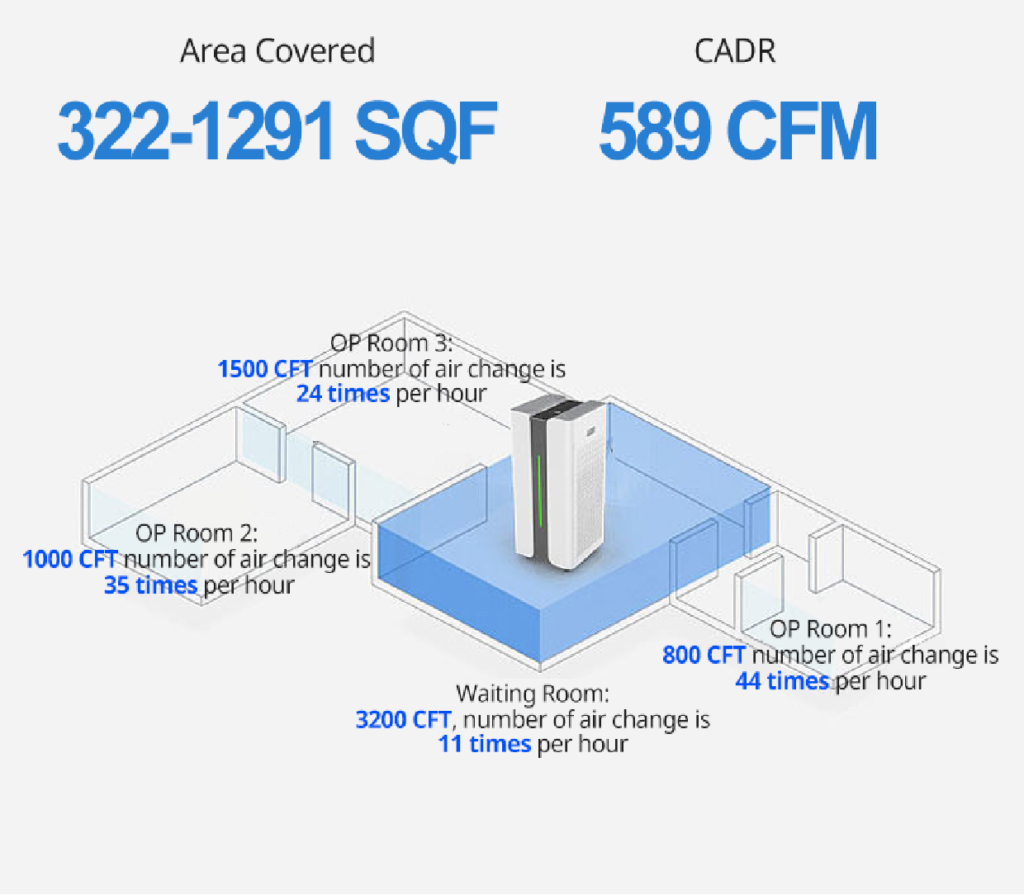
An air purifier’s output is measured as CADR (Clean Air Delivery Rate) expressed in cubic feet per minute. Using the Berk D9L as an example: The CADR for the BERK D9L is 589 cubic feet per minute. That means it takes 1.4 minutes for one complete air exchange to occur, and it completes 44 air exchanges per hour, subject to proper positioning and operation in an enclosed space.
Using the Berk D9L data and based on 44 air exchanges per hour, the time required for removal or settling of aerosols in minutes ( 99.9% efficiency) is approximately 10 minutes based on the formula : t2 – t1 = – [ln (C2 / C1) / (Q / V)] X 60, with t1 = 0. (
Consult an HVAC professional for options to further improve ACH and removal or settling time. See Appendix B, Air Contaminant Removal, attached below.)
Based on: CDC Guidelines for Environmental Infection Control in Health-Care Facilities.
More information here : https://www.cdc.gov/infectioncontrol/pdf/guidelines/environmental-guidelines-P.pdf
Legal Disclaimer: It is not claimed or suggested that this product is safe or effective for the prevention or treatment of COVID-19. Product is not a medical device.
A study from Wuhan hospitals that collected 35 aerosol samples: Air exchange rates in Wuhan Hospital Study on RNA concentration of SARS-CoV-2 Aerosol
This email series is a review of the available evidence for aerosol transmission of SARS-CoV-2 including links to open access journal articles.
Bassel Gebrael DDS, Dip. Perio, FRCD(C)
Part 2: How viable is aerosol transmission of SARS-CoV-2 and how can it be limited?
35 aerosol samples were collected in Patient Areas (PAA) and Medical Staff Areas (MSA) of Renmin Hospital of Wuhan University and Wuchang Fangcang Field Hospital, and Public Areas in Wuhan, China during COVID-19 outbreak.
Polymerase chain reaction was employed to quantitate the viral SARS-CoV-2 RNA genome and determine aerosol RNA concentration.
The ICU, CCU and general patient rooms inside Renmin, patient hall inside Fangcang had undetectable or low airborne SARS-CoV-2 concentration but deposition samples inside ICU and air sample in Fangcang patient toilet tested positive.
Negative pressure ventilation, high air exchange rate, open space, and proper use and disinfection of toilets was found to effectively limit aerosol transmission.

One significant direct source of SARS-CoV-2 in aerosol may be the resuspension of virus-laden aerosol from the surface of medical staff protective apparel as they are being removed and the resuspension of floor dust particles.
This open access reference article is available online to learn more:
Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals during COVID-19 Outbreak. Yuan Liu, Ph.D et al. March 2020 bioRxiv preprint
https://www.biorxiv.org/content/10.1101/2020.03.08.982637v1.full.pdf
