Uncategorized
Flight Defender Aerosol Evacuator

Jun
The regulatory decisions made in the next few months will determine our dental careers. This email series is a review of the available evidence for aerosol transmission of SARS-CoV-2 including links to open access journal articles.
Bassel Gebrael DDS, Dip. Perio, FRCD(C)
Part 1: Understanding mulitphase turbulent gas clouds
The main method of transmission of SARS-CoV-2 is through droplets expelled from the mouth when coughing, sneezing and talking, but there is new evidence of transmission through aerosol which can persist in the air longer and travel further than droplets.
Droplets versus aerosols:
Carl Flugge in 1897 recognized that pathogens were present in expiratory droplets and that “Droplet transmission” could occur through contact with infected droplets.
Large droplets settle before undergoing significant evaporation and contaminate the immediate surroundings of the infected individual.
Smaller droplets evaporate quickly as they transition from the warm and moist respiratory system into the cold and dry air in the environment. The evaporated droplets form residual particles referred to as droplet nuclei or aerosols.
The World Health Organization and the Center for Disease Control have classified routes of disease transmission based on droplet diameter cutoffs from 5 to 10 micrometers. They categorize transmission as “droplet” versus “aerosol” route.
Gas Clouds: A new model for understanding respiratory transmission:
Recent studies have demonstrated that exhalation, sneezes and coughs are made of a multiphase turbulent gas cloud that carries within it ambient air and a continuum of droplet sizes. The moist and warm gas cloud allows droplets to resist evaporation for several minutes and preserves the forward momentum of emission. Droplets in the gas cloud evaporate or settle on surfaces at various rates dependent on temperature, humidity, and air flow patterns.
Droplets that settle contaminate surfaces, and droplets that evaporate produce droplet nuclei (aerosols) that can stay suspended in the air for hours and result in viable virus particles at a great distance from patients.
How far away is safe?
Recommendations from WHO to maintain a 1 meter distance away from symptomatic patients, and the CDC recommendation of a 2 meter separation may not account for the longer range of a high momentum gas cloud and the potential for health care workers to be exposed at greater distances from patients
Are masks and respirators effective against high-momentum pathogenic gas cloud?
The protective efficacy of N95 respirators and surgical masks depend on the ability of the mask to trap the high-velocity gas cloud produced by exhalation or by dental high speed instruments. There is limited data on their efficacy in withstanding prolonged exposure to a high velocity nebulized pathogenic aerosol.
This open access reference article is available online to learn more:
Turbulent Gas Clouds and Respiratory Pathogen Emissions: Potential Implications for Reducing Transmission of COVID-19. Bourouiba L JAMA. 2020 Mar 26
https://jamanetwork.com/journals/jama/fullarticle/2763852
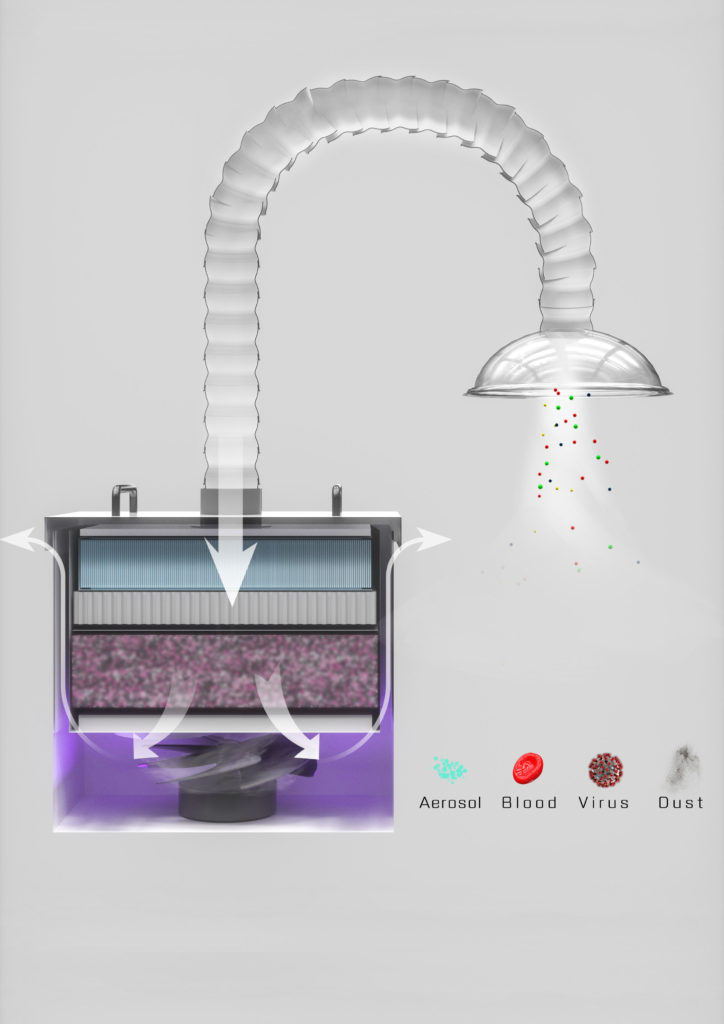
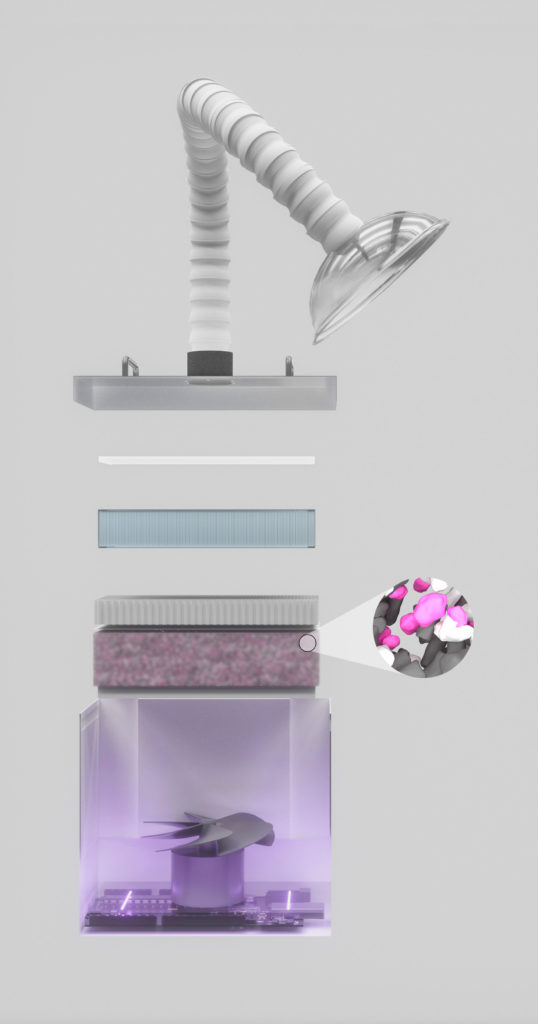
Now available to order: Flight Defender Aerosol Evacuator.
Reserve yours today: Supply bottleneck is expected.
Achieve effective chair side filtration through a 3 stage HEPA filter with 99.97% efficiency and Ultraviolet C disinfection.